Introduction
Comprehensive introductory plans and the availability of subsidized or free healthcare given by the Venezuelan government in the 1980s and 1990s made the country’s health care system among the most developed in the region. By 2000, a large population of people both in towns and rural areas could access clean water and better sanitation. With a high life expectancy of 74, the Venezuelan healthcare system would be expected to be above average.
However, from the 1980s, the once intensive and well-financed medical system in Latin America underwent a sharp decline. The fast collapsing system has been marred by incompetence, poor services, dissatisfied personnel, decaying infrastructure, and a drain of trained medical staff. Allegations of politicizing the system continue flying among interest groups while the Chavez government remains adamant in making the necessary healthcare reforms.
Even with free public healthcare, private medical care is first gaining prominence. This paper presents a critical evaluation of the Venezuelan healthcare system by analysing its current status regarding life expectancy, mortality rates, national health policies, availability, distribution and quality of healthcare all in line with the Millennium Development Goals. Major healthcare challenges and an assessment of its sustainability in the fast-changing global healthcare system will also be discussed.
Status of Health Care in Venezuela
The Health and Social Development Ministry (HSDM) is charged with providing health care in Venezuela and the VISS is the state social security institute that gives medical coverage for over 60% of the Venezuelans (Wilpert, 2006, p. 55). The face of healthcare in Venezuela greatly transformed in the 1980s following comprehensive and progressive vaccination systems and subsidized health care services. According to the WHO 2009, the entire population stood at 28,583,000 with a life expectancy of 71 years for men and 78 for women; a big improvement from 43 years in the 1940s (WHO, 2009).
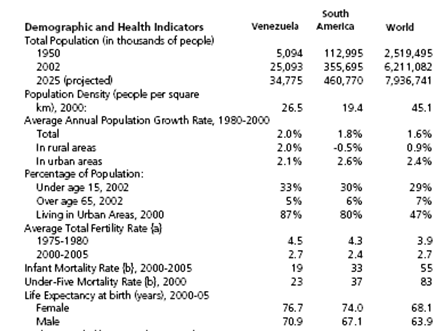
However, health care spending dropped drastically in the 1990s as a result of macroeconomic instability and excessive dependence on oil to sustain expenditure. It has remained steady since 2000 at 3.9% of the GDP making it one of the lowest healthcare expenditures in Latin America (Nichols & Morse, 2010, p. 112). The fundamental health care indicators: life expectancy and infant mortality have stayed almost in sync with the entire region as demonstrated in the figure below.
Life Expectancy and Mortality Rate
According to the CIA World Fact Book 2009, life expectancy was rated at 74 and one out of five Venezuelans had private health cover (the United States Central Intelligence Agency, 2009). The mortality rate dropped considerably to 4 for every 1000 people. Infant mortality also fell to 27 deaths for every 1000 births. However, there are comparatively high occurrences of diseases more so in neglected urban areas and rural regions as a result of malnutrition and substandard sanitation and housing. This has also been accelerated by urbanization and change to inactive employment leading to a rise in lifestyle diseases especially cardiovascular disease which is the championing cause of death in the country (Schargrodsky & Hernández-Hernández, 2009, p. 59).
Contagious diseases especially dengue fever, TB, malaria and measles have resurfaced in recent times. HIV/AIDS is also common though its real degree is undetermined. A campaign was launched by President Chavez in 2001 to combat the dengue fever menace (Brouwer, 2011, p. 113). The rigorous efforts have borne some fruits in the monitoring and successive abatement of infectious diseases.
Public Versus Private Healthcare
The Venezuelan government invested a substantial amount in subsidized and free healthcare in the 1980s making the country a point of reference among its neighbours (Wilpert, 2006, p. 13). However, this huge investment has slowly dwindled. The healthcare system continues to worsen alongside other public sectors while the private sector continues to excel. Though the government by 2002 had reinvested 4.1% of its GDP in healthcare, the figure is still down and decreases with every budget (IMF, 2008, p. 555).
Private insurance has thrived in the past ten years and its quality can be tantamount to the United States. It currently serves half of the population in general hospital bed accommodation and expenditure. It has continued to grow just as apprehension about state healthcare continues to mount since a considerable number of people are moving towards purchasing private health cover. However, private healthcare providers are expensive, and more profit oriented as the cost of private insurance far surpasses its neighbours’.
While there still is free health care for all, there has been anxiety over the investment and quality of services. According to Westhoff, Rodriguez, Cousins and McDermott (2010), it is estimated that 2,000 doctors left Venezuela’s public sector between 2006 and 2008 in protest of the treaty with Cuba (p. 526). This, alongside the looming threat of collapse, demonstrates the big and widening gap between the public and private healthcare sectors in the country and the obvious challenges in the region.
Health Policy Outline
The Venezuelan constitution provides for rights to healthcare. Just like in other Latin American nations, Venezuela lacks qualified and approved medical staff. In an attempt to reach and serve rural and poor communities, the Venezuelan government signed a trade treaty with Cuba in 2003 offering free healthcare services to Venezuelans in exchange for discounted oil (Westhoff, Rodriguez, Cousins, McDermott, 2010, p. 520). The government in 2003 initiated Barrio Adentro; a widespread yet contentious healthcare program aimed at supervising and controlling disease and statistical data in diagnosing and moderating the outbreak of contagious diseases.
The concept incorporates standardized sections of the health system with personnel providing free services to call 24/7. Following this program, 8,000 clinics have been constructed in needy regions availing primary remedial and protective health services. It is a participatory healthcare system that also encompasses health advocating and prevention presentations (Maybarduk, 2004, p. 1). Gradually, the 1.5 million dollar project has grown to avail a wider range of clinics and hospitals for the entire Venezuelan population and also train the natives. As Cruz and Ramón (2008) report, the concept also encompasses urgent medical services, optometrists, psychoanalysis, operations, cancer management oral and dental attention, complementary eye clinics, aid mechanisms for the disabled and admission to an array of medical personnel (p. 36).
Key Challenges
Since the 1990s, the country’s healthcare system has undergone a drastic decline from among the most intensive, well-financed system in Latin America to a disintegrated, underfunded program. This was further sabotaged by an incomplete decentralization operation initiated in the 1990s (Veltmeyer, 2004. p. 114). While the 1999 Venezuelan constitution provides for the right to free medical services, the reality is that public hospitals are disorganized, underfinanced and substandard. Underpaid medical personnel take part in regular strikes demanding better pay and salary arrears. Similarly, healthcare provision is centred in urban areas at the expense of rural and marginalized regions (Mesa-Lago, 2008, p. 172).
The Chavez administration also faces a lot of criticism from international parties. While the government investment in public healthcare is apparent, private medical care has been blamed for profiteering at the expense of services. Anxiety over the National Health Service sustainability and services has seen many citizens resort to private healthcare. The economic recession has not helped as the country in 2011 was obliged to cut down on healthcare expenditure by 1% (Wilpert, 2006, p. 98). The current adulteration in the healthcare infrastructure, services and the inadequacy of drugs may go on if urgent changes are not made.
The Barrio Adentro program has also come under a lot of criticism. Its dependence on doctors from outside poses debates about its long-term sustainability. Healthcare reforms and policies are also points for nonstop political strife between the government and various interest groups. Ewell (1984) observed that some outpatient centres are understocked and lack expert healthcare personnel (p. 225).
There have been calls for a privately managed, state supervised healthcare and annuity program, a move which the president is reluctant to launch. The VISS also requires urgent reforms as its hospital and outpatient insurance structure is regionally disproportionate. Nevertheless, the Venezuelan government is bequeathing a lot in establishing its recommended basic healthcare structure; a venture that would greatly relieve the hospitals’ load through managing diseases before they demand hospitalization (Nichols & Morse, 2010, p. 123).
The Future of the Health Care System
Venezuela was at one time an example of how to invest in a country’s health system and despite the challenges; the country is still among those countries with enviable mortality and life expectancy rates and a comparative health care system. The need for medical services and products is predicted to increase in the coming five years owing to the population boom and growing life expectancy.
Veltmeyer (2004) believes that the less popular government is expected to increase healthcare expenditure (p. 6). However, there is mounting anxiety on the great disparity between private and state health care services and infrastructure. The one-time state of the art hospitals have been reduced to shambles and while free medical care for all exists, it is more in theory since its quality and availability differs from one region to another. Just like in other nations worldwide, Venezuelans who can afford private medical cover are growing in numbers and private healthcare is likely to take over completely (Briggs & Mantinni-Briggs, 2009, p. 549).
Conclusion
The health care sector in Venezuela appears to move in a different direction compared to other countries in the region. While Venezuela at one time was leading in investing substantially in health care, the situation is different now with lowered actual investment in the health department. The country has lost its competitive advantage and can barely manage to keep up with others in the region. Owing to underinvestment in public healthcare, private healthcare is fast taking over in the country while reforms that would see a reprieve in the sector and keep up the recommendable job of the 1980s are yet to be accomplished.
References
Briggs, C.L. & Mantinni-Briggs, C. (2009). Confronting health disparities: Latin American social medicine in Venezuela. American Journal of Public Health, 99(3) p. 549– 555.
Brouwer, S. (2011). Revolutionary doctors: how Venezuela and Cuba are changing the world’s conception of healthcare. New York, NY: NYU Press.
Cruz, E. R.B. & Ramón, S. S.P. (2008.) National Training Program for Comprehensive Community Physicians, Venezuela. MEDICC Review, 10(4) p. 35- 41.
Ewell, J. (1984). Venezuela, a century of change. Stanford, CA: Stanford University Press.
International Monetary Fund. (2008). Government Finance Statistics Year book, Volume 31. Washington, D.C: IMF.
Maybarduk, P. (2004). A people’s health system: Venezuela works to bring healthcare to the excluded. Multinational Monitor: Third world Traveller. Web.
Mesa-Lago, C. (2008). Reassembling social security: A survey of pensions and healthcare reforms in Latin America. Oxford: Oxford University Press.
Nichols, E.G. & Morse, K. J. (2010). Venezuela. Santa Barbara, CA: ABC- CLIO.
Schargrodsky, H.R. & Hernández-Hernández, R. (2009). CARMELA: Assessment of Cardiovascular Risk in Seven Latin American Cities. The American Journal of Medicine, 121(1), p. 58-65.
United States Central Intelligence Agency. (2009). The World Fact Book of 2010. Washington, DC: Potomac.
Veltmeyer, H. (2004). Globalization and antiglobalization: dynamics of change in the new world order. Surrey, UK: Ashgate Publishing.
Westhoff, W.W., Rodriguez, R., Cousins, C. and McDermott, R.J. (2010). Cuban Healthcare Providers in Venezuela: A case study. Public Health, 124(9), 519- 524.
Wilpert, G. (2006). Changing Venezuela: The history and policies of the Chavez government. New York, NY: Verso.
World Health Organization. (2009). World Health Organization Assesses the World Health Systems. Web.
